AS Psych: Saavedra and Silverman (button phobia)
Psychology Being Investigated
1. Evaluative learning occurs when a previously neutral stimulus or event is now perceived negatively
– The person negatively evaluates the object/event without anticipating a threatening outcome like in expectancy learning, thus eliciting a feeling of disgust rather than fear
2. Operant conditioning is learning through the consequences of our actions e.g. using a reward to reinforce a certain behavior
3. Classical conditioning is learning through association
4. A phobia is an irrational and persistent fear of an object or event that poses little danger but creates anxiety and avoidance in the sufferer (it can be learned and unlearned)
Background
Merckelbach et al.
– Found negative evaluation elicits disgust rather than fear
De Jong et al. (1997)
– Investigated children with spider phobia
– Found disgust reduced alongside fear reduction
Aims
1. To investigate the cause of a boy’s button phobia to see if disgust is involved.
2. To test the effectiveness of exposure therapy for a button phobic by targeting disgust and fear.
Method
Research Method: Case study (using interviews, self-report, and observation)
Sampling technique: Opportunity
Sample
– 9 year old
– Hispanic American boy
– Had button phobia since the age of 5
– Diagnosed with button phobia using DSM-IV
Procedure
History
– When he was 5, the boy ran out of buttons for an art project
– Asked to come to the front to get more buttons, which were in a bowl on the teacher’s desk
– Distressing experience: his hand slipped, and all the buttons in the bowl fell on him
– Button avoidance continually increased, until it affected his normal life (cannot concentrate in school, avoid clothes with buttons, etc.)
Interview and diagnosis
– Informed consent obtained from the boy and his mother
– Interviewed boy and his mother about phobia
– DSM-IV used to confirm diagnosis of button phobia → did not meet requirements for OCD!
Behavioral Exposure Therapy
– Contingency management: boy received positive reinforcement from his mother, upon successful completion of each exposure to buttons
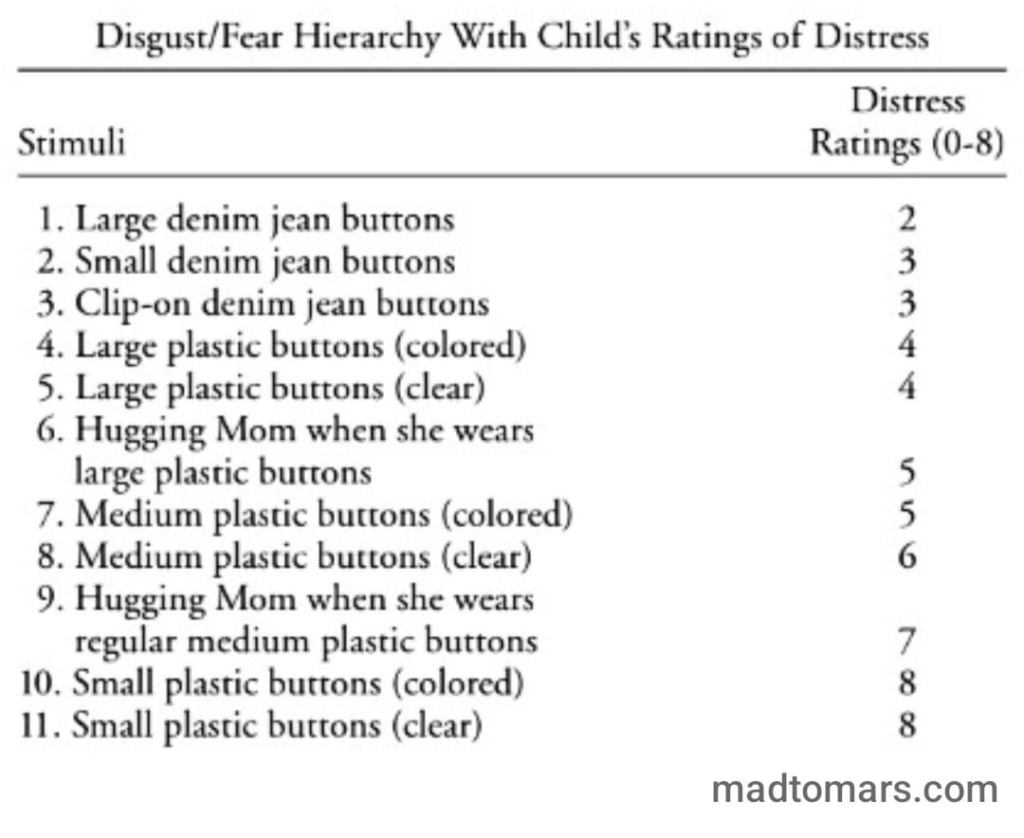
– Disgust/Fear hierarchy created + boy’s subjective rating of distress (9-point scale, used Feelings Thermometer)
– 4 sessions to complete hierarchy list (each session 30 mins with boy + 20 mins with mom)
– However, ratings of distress continued to increase
Image Exposure Therapy
– Upon further probing, it was found that the boy found buttons disgusting upon contact with his body + that buttons emitted unpleasant odors
– Used self-control/cognitive strategies
– Asked to imagine buttons falling on him + describe how they looked, smelled, felt + elaborate on how they made him feel
– Progressed from smaller buttons to larger buttons
– 7 sessions to complete hierarchy list
– Overall: ratings decreased
Results
Behavioral exposure
– Completed all in vivo (real life) exposure tasks
– Could handle more buttons after 4 sessions
– BUT distress increased (severity rating 6 to 8)
Image Exposure
– Ratings of distress decreased during session
– “Imagine buttons falling all over his body” (severity rating before: 8, midway: 5, after: 3)
– “Hugging mother with a shirt full of buttons” (severity rating before: 7, midway: 4, after: 3)
6 and 12 month follow-up
– No longer classified under DSM-IV for specific phobia
– Reported minimal distress about buttons
– Able to resume normal activities in school
Conclusion
1. A phobia can be treated with positive reinforcement and imagery/behavior exposure.
2. Disgust does play a crucial role in the development and maintenance of button phobia.
Ethical Issues
Protection from Harm – the boy may have been distressed when exposed to the buttons
Informed consent – both the boy and mom consented to participate in the assessment and intervention procedures
Application to Daily Life
– Phobias can be treated using imagery exposure (letting patients think about their phobia in order to find them less distressing) and behavioral exposure (gradually exposing patients to their phobia)
– For children with phobias, having a parent involved in the therapy might bring about faster positive outcomes